
Audiometry Simulator
Take the virtual patient into the sound booth, place the headphones and present the stimulus yourself. Find air- and bone-conduction thresholds with the Hughson-Westlake procedure; notice cross-hearing, mask the non-test ear, do not skip the inter-octave frequencies. When you are done, compare your audiogram with the true thresholds, see your errors and download your clinical report.
Works on desktop and tablet · headphones recommended
- 10 clinical cases
- 3 practice modes
- Air + bone conduction
- Masking
- PNG / PDF report
Before you begin
Four short notes, so that you get sound results from the simulator and protect your own hearing.
Desktop or tablet
The simulator does not open on a phone screen: the console, the booth and the audiogram cannot fit on one small display, so small screens are deliberately blocked. Hold your tablet in landscape.
Headphones preferred
The stimulus is delivered to one ear; with speakers the right/left distinction and masking lose their meaning. The headphones are not calibrated — the levels are only relatively correct.
Raise the volume gradually
The audiometer goes up to 120 dB HL; above 100 dB the screen asks for a warning confirmation. Start with your system volume at a moderate level and raise it slowly if needed.
For education only
This is a simulation; it is not a diagnostic tool, a calibrated audiometer or a hearing test. The report it produces is not a medical document.
How does it work?
The flow of a real pure-tone audiometry session: pick the case, present the stimulus, record the threshold, compare the result.
-
1
Choose the case and the mode
Pick one of the 10 clinical cases, or the blind case. There are three practice modes: Free (unlimited attempts), Guided (rule reminders on) and Exam (no hints; time and errors are counted). If you like, start with the Weber–Rinne tuning-fork screening.
-
2
Choose the transducer, present the stimulus
Supra-aural or insert? Your choice changes the masking rules (interaural attenuation of 40 dB versus 60 dB). Select the ear and the frequency, then press the PRESENT TONE button with a short + long rhythm. The patient responds only to a properly presented stimulus.
-
3
Find the threshold, mask when needed
Down 10 dB, up 5 dB. Record the threshold once at least half of the presentations get a response — the simulator checks the Hughson-Westlake criterion and warns you if you record too early. If you suspect cross-hearing, present narrow-band noise to the non-test ear and find the true threshold with the plateau method.
-
4
Compare and take your report
When you finish, your audiogram is overlaid on the true thresholds: where you forgot to mask, where you recorded a shadow curve, which inter-octave frequency you skipped — each one is shown. Then download your A4 clinical report as a PNG or a PDF.
Cases
Ten cases, ordered by difficulty, from normal hearing to the Masking Dilemma. The diagnoses are not spelled out here — you are the one who will interpret the case.
There is also a Blind Case option: you test without knowing the pathology and find out at the end.
Controls and shortcuts
You can drive the console with the mouse, but the keyboard is much faster. Inside the simulator you can open this card at any time by pressing ? .
Keyboard shortcuts
| Space | Present the stimulus (hold) — with a short + long rhythm |
| ↑↓ | Raise / lower the level by 5 dB |
| ←→ | Change the frequency |
| Enter | Record the threshold |
| N | Mark as no response |
| C | Silent control trial (reliability) |
| M | Turn masking on / off |
| RL | Switch to the right / left ear |
| ? | Open the shortcut card |
| Esc | Close the open window |
What is on the console?
-
EarRight / left selection; the symbol and the colour change automatically.
-
PathwayAir conduction, bone conduction, sound field (speaker) and UCL measurement.
-
StimulusPure tone or warble; pulsed or continuous.
-
TransducerSupra-aural / insert; it directly changes the masking rules.
-
Masking dialNarrow-band noise to the non-test ear; you set the level.
-
Learning panelRule reminders and warnings in Guided mode.
Tip: while presenting the stimulus you can change the level with ↑↓ without releasing the button; the patient only responds to a properly presented stimulus.
Audiogram symbols
The simulator uses the internationally accepted symbol set. The right ear is red and belongs to the circle family, the left ear is blue and belongs to the cross family; masked measurements are boxed.
maskedBoneBone
maskedNo response
Masking rules — a summary
The simulator's engine follows these rules; in the learning mode it warns you when you break one.
| Rule | Supra-aural | Insert |
|---|---|---|
| Interaural attenuation (IA)The level the sound loses while crossing the head | 40 dB | 60 dB |
| When air-conduction masking is requiredThe difference between the AC threshold of the test ear and the BC threshold of the non-test ear | ≥ 40 dB | ≥ 60 dB |
| When bone-conduction masking is requiredIn bone conduction IA is taken as ≈ 0 — the transducer makes no difference | Air-bone gap > 10 dB or Between the BC thresholds of the two ears, a difference of ≥ 10 dB | |
| Occlusion effectThe improvement of bone-conduction thresholds at low frequencies when the ear is occluded | 250 Hz30 dB 500 Hz20 dB 1000 Hz10 dB | 250 Hz10 dB 500 Hz10 dB 1000 Hz0 dB |
The plateau method
Raise the masking noise in steps. If the threshold of the test ear stays unchanged for a while (the plateau), you have reached the true threshold. If the threshold keeps rising with the noise, you are either still on the shadow curve (under-masking) or you have moved into over-masking.
The masking dilemma
With large bilateral air-bone gaps, any adequate masking inevitably suppresses the test ear as well: no safe window is left between under-masking and over-masking.
is usually to switch to insert earphones. Once IA rises from 40 dB to 60 dB, the plateau window opens. You will live through this in the simulator's "Bilateral Conductive" case.
The clinical report
When you finish the test, your measurements are laid out on a real clinical form.
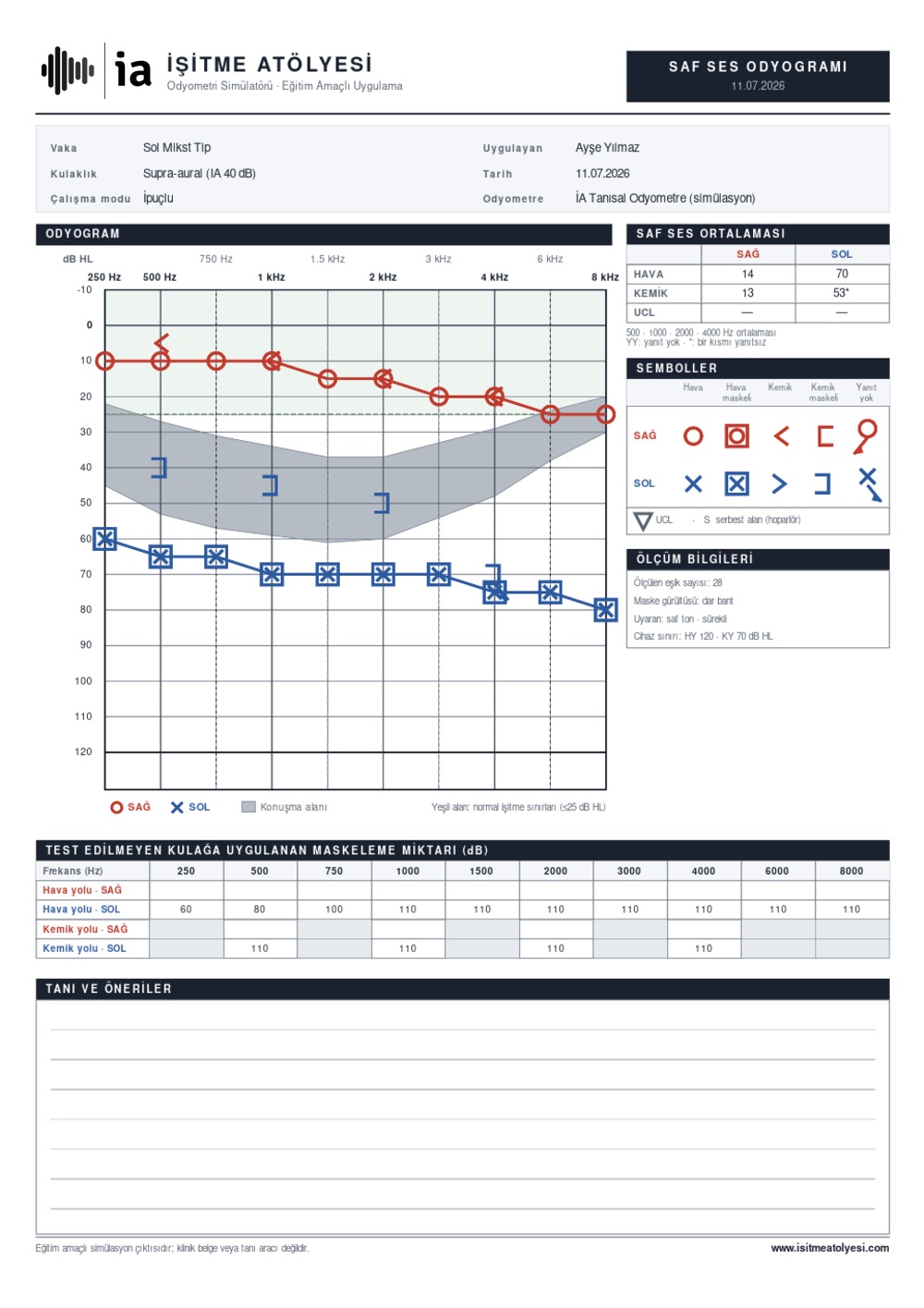
The report follows the layout of a real clinical form: header details, audiogram, averages, masking table and an open assessment area. It is printed as vector graphics, so it stays sharp on paper.
- AudiogramPlotted with the standard symbols; the normal hearing range and the speech banana are shaded.
- Pure-tone averageRight/left PTA for air and bone conduction; if you measured UCL, it is in the table too.
- Masking tableThe amount of masking delivered to the non-test ear at each frequency.
- Header detailsCase, transducer, practice mode, the name of the tester and the date.
- Symbol legendTogether with the measurement details: stimulus type, masking noise, device limits.
- Diagnosis and recommendationsAn area left blank — you can fill it in by hand and hand it in.
For instructors
The simulator was built for the classroom: you can open a student's whole session from a single code and design the scenarios around your lesson.
How does classroom mode work?
- 1The student finishes the testThe case, the mode and every measurement stay in their browser.
- 2A classroom code is generatedA short text code that encodes the entire session.
- 3You decode itPaste the code into the decoder in the simulator and the session opens in front of you.
What is inside the code: which case, which mode, which thresholds, how many errors, the masking decisions and the response reliability.
No data is sent to any server. The code is generated in the student's own browser; sharing it is entirely up to them.
Ideas for the classroom
-
Warm-up
The Normal Hearing case with Guided mode. The aim is to learn the method, not to make a diagnosis.
-
Teaching the rules
Have them run the Left Severe SNHL case without masking first; discuss the shadow curve together, then have them repeat it with masking.
-
The Masking Dilemma
Give them the Bilateral Conductive case with supra-aural phones. When they get stuck, ask them to switch to inserts.
-
Assessment
Exam mode plus the classroom code. Give them the blind case and ask for the report and the interpretation together.
-
Homework
Have them complete the "Diagnosis and recommendations" section of the downloaded A4 report.
Frequently asked questions
You start with the better ear and at 1000 Hz. From an audible level you proceed in down 10 dB, up 5 dB steps (the modified Hughson-Westlake procedure). If a response is obtained on at least half of the presentations at the same level (typically two out of three), that level is the threshold.
The usual order is 1000 → 2000 → 4000 → 8000 → (1000 again) → 500 → 250 Hz. Repeating 1000 Hz is a reliability check: if it differs from the first measurement by more than 5 dB, the test is repeated. Once air conduction is done, bone conduction is measured.
In air conduction: if the difference between the air-conduction threshold of the test ear and the bone-conduction threshold of the non-test ear is equal to or greater than the interaural attenuation (40 dB with supra-aural phones, 60 dB with inserts), the sound can cross the head and be heard in the better ear — masking is required.
In bone conduction: the sound reaches the opposite cochlea with almost no attenuation (IA ≈ 0). So masking is used whenever the test ear shows a meaningful air-bone gap (> 10 dB) or the bone-conduction thresholds of the two ears differ by ≥ 10 dB.
When you present a loud sound to the poorer ear, it vibrates the skull and can be heard in the better ear. The patient responds, but not with the ear you are testing. The misleading curve you plot without masking is called the shadow curve ; it typically runs parallel to the better ear's thresholds, one IA (40–60 dB) below them.
The unilateral profound loss case in the simulator sets exactly this trap: without masking you will find a "60 dB threshold in the left ear" — while the left ear hears nothing at all.
It is the standard up-down staircase used to search for a threshold. After a response the level is dropped by 10 dB; after no response it is raised by 5 dB. This "down 10 / up 5" oscillation produces repeated ascending approaches to the threshold. The threshold is defined as the lowest level at which a response is obtained on at least 50% of the ascending trials .
The simulator runs this check in the background: if you record a threshold without enough repetitions, it warns you.
If the thresholds of two neighbouring octaves differ by 20 dB or more, the half-octave frequency in between is measured as well. Otherwise the real shape of the curve is missed — in a noise notch in particular, skipping 3000 and 6000 Hz hides the notch completely.
To mask during bone-conduction testing you place a phone on the non-test ear. When the ear canal is closed, the bone-conduction threshold at low frequencies improves — that is, the patient hears better than expected. This gain has to be added when the masking level is calculated.
The effect is marked with supra-aural phones (~30 dB at 250 Hz) and very small with deeply seated inserts. It appears in ears with a normal middle ear; in a conductive loss it is not expected, because a "natural occlusion" is already present.
The noise in the non-test ear becomes so loud that it too crosses the head and starts to mask the test ear. The threshold of the test ear then worsens artificially. The safe window between under-masking and over-masking is called the plateau ; the true threshold lies there.
No. The simulator runs entirely in your browser; no measurement is sent to a server. Your progress is kept only in your own browser's local storage. The classroom code is generated in your browser too — whether you share it is up to you.
The audiometer console, the view of the booth and the live audiogram all have to be on screen at once. At phone width that layout stops being usable; pressing the wrong key and recording the wrong threshold becomes far too easy. Small screens are therefore blocked on purpose. A tablet works in landscape.
No. What is tested here is a virtual patient; you are the tester. The sounds are not calibrated and depend on your computer's volume, so draw no conclusions about your own hearing. If you have concerns about your hearing, see an audiology clinic.
Sources
The simulator's acoustic model, masking rules and threshold-search procedure are based on the standard sources below.
- Katz, J. (Ed.). Handbook of Clinical Audiology. Wolters Kluwer.
- Yacullo, W. S. Clinical Masking Procedures. (Clinical masking, the plateau method and the masking dilemma.)
- Gelfand, S. A. Essentials of Audiology. Thieme.
- Roeser, R. J., Valente, M., & Hosford-Dunn, H. (Eds.). Audiology: Diagnosis. Thieme.
- British Society of Audiology. Recommended Procedure: Pure-tone air-conduction and bone-conduction threshold audiometry with and without masking.
- American Speech-Language-Hearing Association (ASHA). Guidelines for Manual Pure-Tone Threshold Audiometry.
- Carhart, R., & Jerger, J. F. Preferred method for clinical determination of pure-tone thresholds. Journal of Speech and Hearing Disorders. (The source of the modified Hughson-Westlake procedure.)
- ISO 8253-1. Acoustics — Audiometric test methods — Part 1: Pure-tone air and bone conduction audiometry.
If you are ready, step into the booth
If you spot an error, if a rule behaves incorrectly, or if there is a case you would like added, write to us: info@isitmeatolyesi.com. The simulator is an open-ended educational project; it grows with feedback.