In this article, we discuss the paper titled "Why Extended High-Frequency (EHF) Hearing Assessments Are Necessary," published in Hearing Tracker in January 2026 by Dr. Douglas L. Beck, Dr. Melissa Fling and Dr. Keith N. Darrow.
Hearing loss, which affects approximately 1.5 billion people worldwide, is one of the most common neurological conditions. Although traditional estimates put the figure at 38–45 million people in the U.S., the recent Global Burden of Disease Study reports that this figure has reached 73 million, affecting 22% of the population. More critically, about 26 million Americans experience "subclinical" listening problems despite having normal pure-tone thresholds.
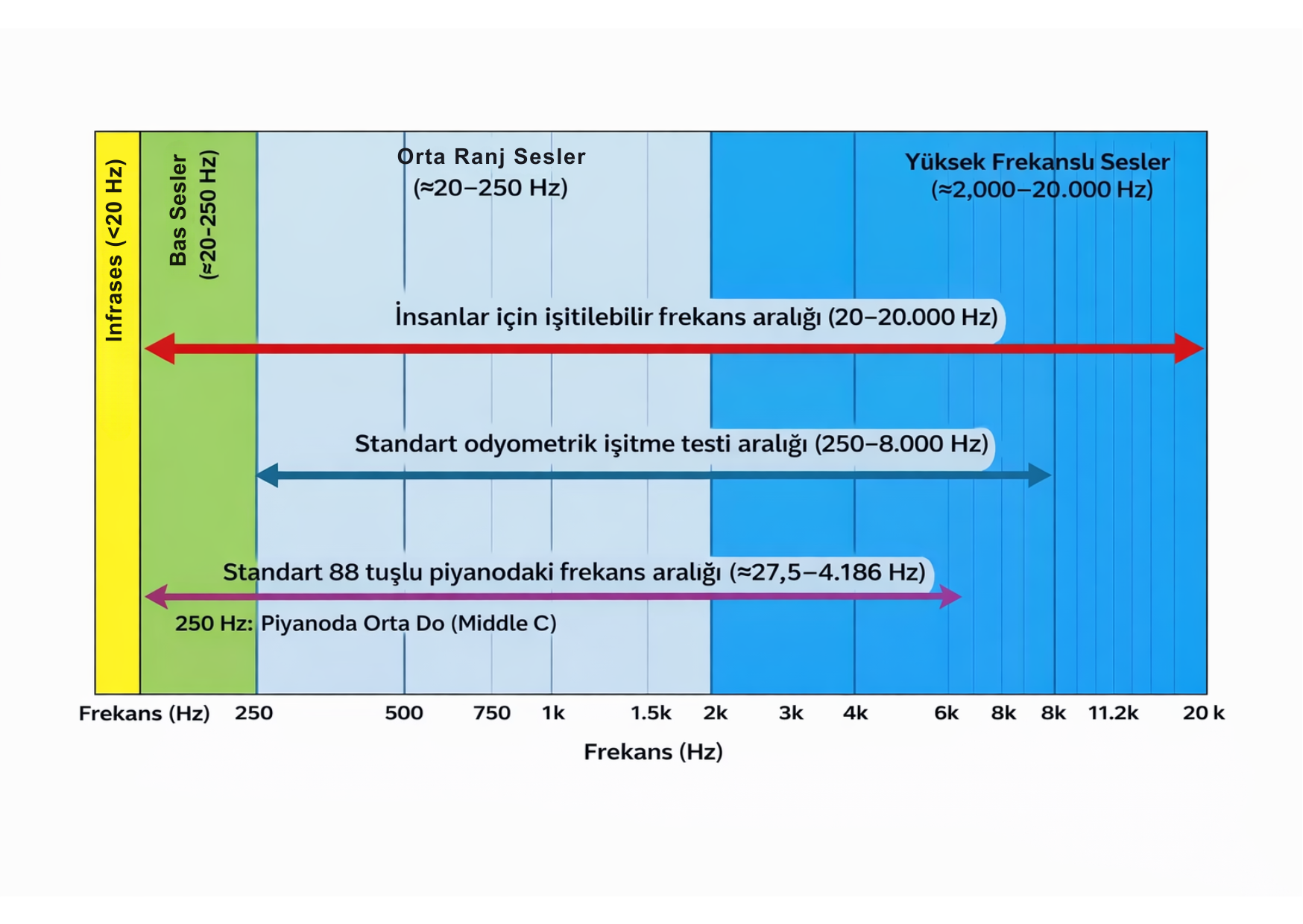
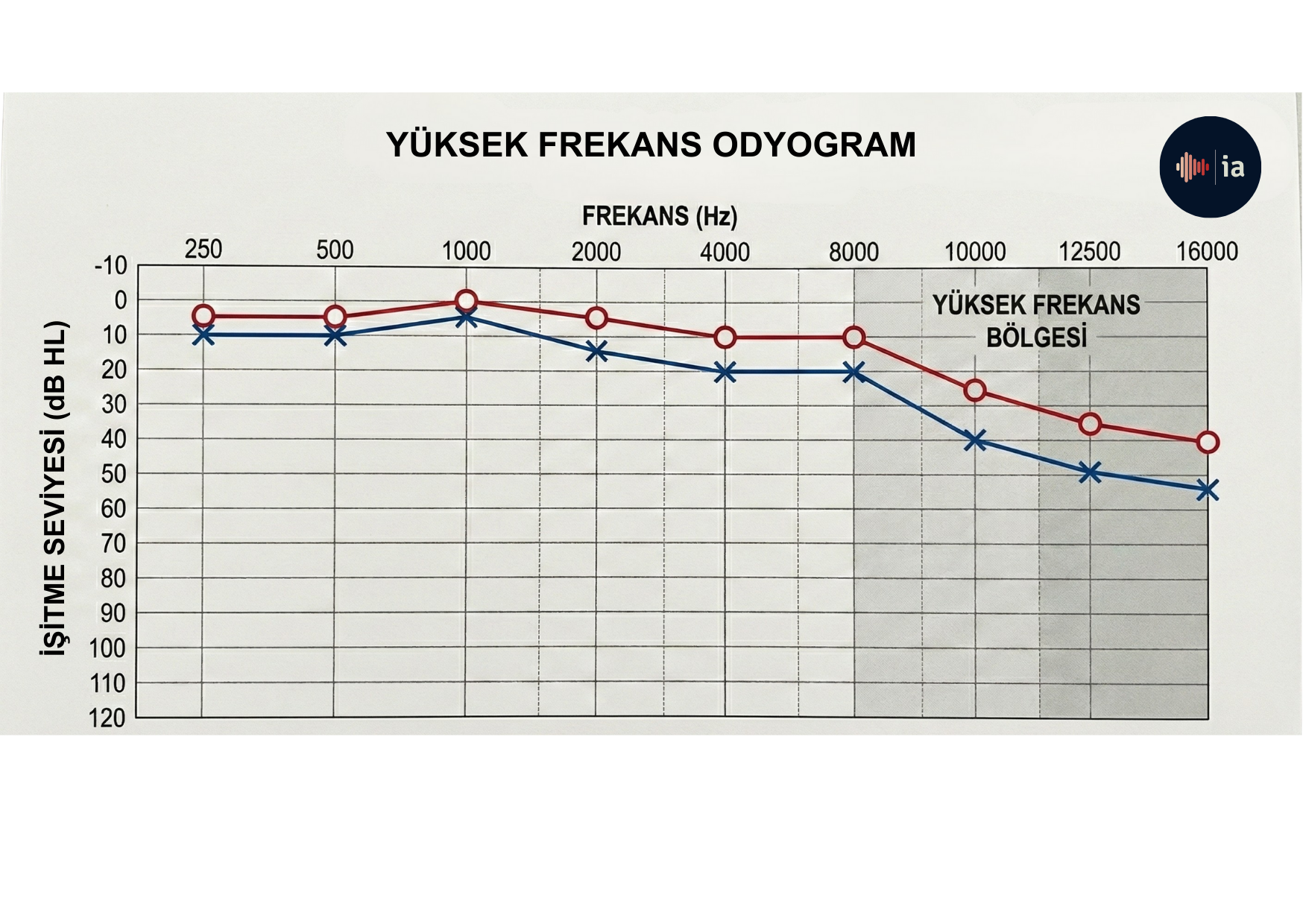
Pure-tone audiometry, regarded as the "gold standard" for about 100 years, is successful at measuring sensitivity from 250–8,000 Hz; however, it does not fully reflect the functional capacity of the dynamic auditory system. Hearing is the passive perception of sound, while listening is the brain making sense of sounds. Telling a patient "your hearing is normal" only indicates that thresholds up to 8 kHz are within norms; it does not mean that auditory processing is healthy.
What does this mean? Patients' complaints of "I hear but I don't understand" or "people are mumbling" may be related to the loss of spectral cues above 8 kHz or to disruptions in neural synchronization.
The human auditory system uses spectral cues, particularly between 4–16 kHz, to determine the location of sound in space: 6–12 kHz contributes to vertical localization, and 8–16 kHz to front-back discrimination. This information is not visible on the standard audiogram.
Even if 75–80% of cochlear nerve fibers have degenerated, pure-tone thresholds measured in a soundproof booth may come out normal. This is directly related to cochlear synaptopathy and auditory neuropathy, which explain patients' complaints of difficulty understanding speech in noise, tinnitus and increased listening effort.
We have actually had the ability to test up to 16 kHz for a century. The Western Electric 1A model, produced in the 1920s, could measure in the 32 Hz–16,384 Hz range; however, cost and the fact that subsequent portable models were limited to 8,192 Hz confined clinicians to this narrow range.
Adding EHF tests to the routine battery provides high diagnostic yield at low cost. Cases where it is critical include revealing the hidden deficits of tinnitus, early cochlear involvement in genetic/systemic diseases, the first signs of noise damage, increased listening effort, phoneme discrimination and language development in children, and predicting performance in noise. Indeed, thresholds at 16 kHz can reliably predict success in noise even when there is no high-frequency cue in the stimulus.
Modern science has shown that a bandwidth of up to 13 kHz is necessary for speech quality and intelligibility. As audiologists, we should adopt a comprehensive approach that includes high-frequency hearing testing, speech-in-noise (SIN) tests and suprathreshold measures.
Beck, D. L., Fling, M., & Darrow, K. N. (2026). Why extended high-frequency (EHF) hearing assessments are necessary. Hearing Tracker.
